My Arm Story
 My "Shortarm"
My "Shortarm" |
 The Ulnar Shortening Scar
The Ulnar Shortening Scar
|
Click for Fullsize Pictures
![]()
My Arm Story
|
My "Shortarm" |
The Ulnar Shortening Scar
|
Click for Fullsize Pictures
![]()
At the age of 10 years old, I suffered a blow to my radial head(elbow), which caused my the bone to displace from the joint itself. Although no fracture was apparent, pain as well as a notable reduction in motion was. I recovered to a certain degree, but later surgery would be required. Surgery of this nature has to wait until a person has reached most of his/her growth, as uneven bone growth can occur, causing the hand to grow in an outward position. At 13, I again suffered a blow to the identical area, this time causing extreme pain, surgery was performed shortly thereafter. This procedure is called a "radial excision" or "resection", or more plainly, cutting off the end of your funny bone. As time has gone on, ulnar deviation has become a greater problem, the ulnar is too long as the radius has been shortened, driving into my wrist. The following is part of what I am trying to do about it, finally, some 22 years later, I underwent athroscopic surgery and then ulnar shortening.
Excision: of Radial Head:
--------------------------------------------------------------------------------
- Discussion:
- decision to excise the head of the radius depends associated elbow injuries
as well as the severity of radial head frx;
- it has been determined that the stabilizing effect of radial head comes into play
only when the MCL ligament has been disrupted, which explains why
excision of radial head (w/ no other injury) is not associated w/ instability;
- valgus-varus alignment of the elbow can determine the pattern of force transmission thru the forearm;
- w/ valgus stress, the interosseous membrane plays a minimum role in force transmission;
- most of the force will be transmitted directly from the distal radius thru the radial head - captiellar articulation;
- gripping activities which place a varus stress on the elbow do cause force transmission thru the interosseous membrane;
- w/ varus alignment, there will be minimal contact between the radial head and capitellum;
- Surgical Indications: - isolated type-III frx:
- treated w/ early complete excision;
- this method is preferred to simple removal of displaced fragments;
- early excision is more important for type-III frx than for type-II
fractures since success w/ delayed excision in type iii frx is unpredictable;
- w/ excision of radial head (and nl RU joint support), only approx.
2 mm of proximal radial migration is expected;
- concomitant valgus instability: (due to MCL instability)
- consider replacement w/ Silastic or metallic radial head prosthesis
in order to serve as temporary spacer after repair of MCL &
flexor pronator mass;- Contraindications to Excision:
- concomitant RU joint instability indicates a Essex Lopresti Injury);
- Technique of Radial Head Excision;
- is safely carried out thru a posterolateral incision;
- most vulnerable structure to damage is PIN;
- do not extend incision more than 5 cm distal from epicondyle;
- note that the radial head is covered by a coalescence of the LCL and annular fibers;
- excessive disruption of this ligamentous complex during the radial head
excision may lead to posterolateral instability;
- hence attempt to preserve the distal half of the ligamentous complex over
the radial head as well as to keep the incision slightly anterior;
- Complications of Excision: - proximal migration of radius;
- leads to positive ulnar variance;
- in about 15-20% of patients, there will be more than 1 mm of migration;
- migration more than 4 mm is associated w/ pain;
 The Radial Head
The Radial Head
 Elbow Shot
Elbow Shot
Ulnar Variance:
--------------------------------------------------------------------------------
- Discussion:
- mean ulnar variance is 0.9 mm (range: 4.2 to 2.3 mm);
- functional anatomy: - w/ neutral variance, 80% of load is born by radius and 20% by ulna; - 2.5 mm increase in ulnar varience will increase load borne by ulno-carpal joint from 18% to 42%; - a 2.5 mm decrease in the ulno-carpal variance will decrease the load borne by the ulno-carpal joint to 4.3%; - ref: The distal radioulnar joint. Anatomy, biomechanics, and triangular fibrocartilage complex abnormalities.
- negative ulnar variance is associated w/ Kienbock's disease
- positive ulnar variance is associated w/: - SLD; - ulnar impaction syndrome; - tears of triangular fibrocartilage; - lunotriquetral ligament tears; - previous excision of radial head
- Measurement: - requires zero rotation view: (measured on PA radiograph w/ wrist in neutral supination/pronation); - draw transverse line at the level of the lunate fossa, and a second transverse line at the level of the ulnar head; - the difference indicates ulnar variance; - forearm pronation will increase ulnar variance; - forearm supination will decrease ulnar variance;
Triangular Fibrocartilage Complex: --------------------------------------------------------------------------------
- is ulnar continuation of distal radius & presents concave surface for articulation w/ lunate & triquetrium; - ulnar side of the wrist is supported by the TFCC, which articulates w/ both the lunate and the triquetrum; --------------------------------------------------------------------------------
- Anatomy and Function of the TFCC: --------------------------------------------------------------------------------
- Injury to TFC: - mechanism of injury includes twisting w/ palmar rotation;
- commonly associated with positive ulnar variance crepitus, pain, and tenderness between the ulna and triquetrum; - ulnocarpal impaction syndrome is a common inciting cause of degenerative tears;
- mechanism: - during marked ulnar deviation, compressive load on TFC, particularly w/ positive ulnar variance, may increase markedly; - forced ulnar deviance, such as batting a baseball, subjects the TFC to heavy loads;
- classification: - central perforations are usually due to degeneration process (most common); - these occur in a minority of cases; - displacement of the lunate fossa with the TFFC; - in substance tears of the peripheral rim; - peripheral radial attachments are common, and these are amenable to repair; - include avulsion of TFC from ulnar styloid; - least common, but most amenable to surgical repair;
- associated injuries: - tear in lunotriquetral interosseous ligament; - relatively frequent occurrence; - scapholunate dissociation: - less frequent occurrence; - ulnocarpal impaction syndrome (which can also mimic TFCC tear); - impingement of distal ulna on the carpi; - patients may have increased ulnar variance; - distal radius frx: - injury to triangular fibrocartilage is an often unrecognized element of distal radius fractures; - according to the report by Richards et al 1997 et, TFCC tears occurred in 53% of extra-articular distal radius fractures vs 35% of ulnar fractures; - ulnar styloid frx; - in the report by Richards et al 1997, no correlation between ulnar styloid frx and TFCC tears could be found;
- diff dx: - diff dx includes: ECU tendinitis, occult frx, DJD of the pisoform-triquetral joint, and RU joint instability; --------------------------------------------------------------------------------
- Exam of TFCC Injury:
- tenderness is usually centered about dorsal depression distal to ulnar head, or it may be localized around the ulnar styloid;
- patients may also note tenderness between the triquetrum and the ulnar styloid;
- passive manipulation of the carpus against the head of the ulna w/ wrist in ulnar deviation usually causes pain;
- tenderness against resisted radial deviation will also cause tenderness;
- this should be differentiated from the click of midcarpal instability;
- patients will TFCC tears, often show pain w/ forced forearm pronation and supination;
- pts w/ TFCC tears that are symptomatic often note a painful click during wrist motions;
- have the patient clench and ulnary deviate the wrist, and then repeatedly pronate and supinate the wrist;
- in contrast, patients w/ SLD will have pain and a click when the clenched fist is moved from ulnar to radial deviation;
- piano key sign:
- laxity or instability of the R-U joint w/ controled dorsal palmar shucking;
- when this test is positive (as compared to opposite wrist), then RU instability is present;
- this test is not reliable for diagnosing TFCC tears;
--------------------------------------------------------------------------------
- Triple Injection Arthrography:
- study of choice, but can often miss peripheral meniscus tears;
- identification of tears depends on contrast dye passing thru the radiocarpal and DRUJ;
--------------------------------------------------------------------------------
- Radiographs:
- may reveal avulsion of ulnar styloid, scaphoid frx, distal radius frx, or there may be volar tilt to the lunate and triquetrum (VISI deformity);
- ulnar variance: (requires zero rotation view);
- variable length of the ulna as a positive or negative variance may influence the carpal position;
- wrist w/ more positive ulnar variance tends to be associated with relatively thinner TFC articular disc;
--------------------------------------------------------------------------------
- MRI:
- normal disc: uniform low signal at both the radial and ulnar attachment;
- complete tear: full thickness discontinuity which extends thru the articular disc;
- references:
- The utility of high resolution MRI in the evaluation of the TFCC of the wrist.
HG Potter MD et al. JBJS Vol 79-A. No 11. Nov 1997. p 1675.
--------------------------------------------------------------------------------
- Non Operative Treatment of TFC Injuries:
- placement of forearm in neutral rotation in long arm cast places TFCC in the best alignment for healing;
- marked pronation is to be avoided, because this inclines the ulnar head to displace dorsally;
- supination with imperfect radial fragment reduction may result in palmar subluxation of the ulnar head;
--------------------------------------------------------------------------------
- Operative Treatment:
- patients w/ a symptomatic perforation and an ulnar positive variant should be
considered for an ulnar shortening along with the treatment of the tear;
- ulnocarpal impaction syndrome should be addressed along w/ TFCC tear;
- wafer procedure: - partial excision of TFCC:
- as noted by Menon et al 1997, there is a 30% failure rate of partial TFCC excision when concomitant
ulnar shortening is not performed; - references:
Partial excision of the triangular fibrocartilage complex articular disk: a biomechanical study.
Isolated tears of the triangular fibrocartilage of the wrist: results of partial excision.
Menon J, Wood VE, Schoene HR, Frykman GK, Hohl JC, Bestard EA. J. Hand Surg. 1989. 14-A: 527-530.
Partial Excision of the triangular fibrocartilage complex.
Palmer AK, Werner FW, Glisson RR, Murphy DJ. J. Hand Surg. 1988: 13-A: 391-394.
Tears of the articular disc of the triangular fibrocartilage complex: results of excision of the articular disc.
Imbriglia JE, Boland DS. J. Hand Surg. 1983: 8:620.
- TFCC Repair: - indicated primary for traumatic peripheral ulnar sided TFCC tears; - negative predictive factors for successful repair include concomitant ulnocarpal impaction syndrome (associated w/ degenerative tears) and peripheral radial tears (due to the relative avasucularity of the disc in this region; - some surgeons feel that radial sided TFCC tears are not a significant risk factor for healing after a repair; - arthroscopic evaluation: - determine whether the TFCC has a resilient quality when probed (which is normal); - when the arthroscopic probe elicits gross softness, then a peripheral tear may be present; - peripheral tears are often located at the dorsal ulnar peripheral border; - arthroscopic debridement: - may be indicated for tears occupying the central 2/3 of the disc; - relative contra-indication: positive ulnar variance: - hazards: avoid injury to the dorsal and volar wrist ligaments; - open repair: (for peripheral tear at ulnar styloid); - make a 5 cm longitudinal incision centered over the distal ulna; - take care to avoid the dorsal sensory brach of the ulnar nerve; - dorsal incision in made between the 4th and 5th compartments; - incise the dorsal wrist capsule in line with the incision; - the incision should be extended to the lunotriquetral joint; - a radially based retinacular flap is fashioned; - enter the ulnar-carpal joint (inverted T incision) between EDQ and ECU; - scar tissue surrounding the torn TFCC and its bed are debrided w/ scope; - w/ ulnar positive variance, exposure is facilitated w/ an ulnar shortening procedure (such as the wafer procedure); - likewise, placement of a small lamina spreader in the RU joint may facilitate the exposure; - repair of ulnar detachment: - sutures are then passed thru drill holes made at the medial base of the styloid, which are then placed thru the torn medial edge of the TFCC; - a suture passer can be helpful to pass the suture thru the drill holes; - repair of radial TFCC detachment: - drill holes are made in the ulnar side of the dorsal distal radius, from a dorso-radial to a palmar ulnar direction; - horizontal matress sutures are passed thru the TFCC and are then brought thru the distal radial drill holes; - RU stabilization and closure: - place the arm in neutral rotation or slight supination and insert 2 K wires across the RU joint (or just proximal to the joint); - the TFCC sutures are then tied down; - the radially based retinacular flap is then passed underneath the ECU tendon inorder to help prevent subluxation; - references: Isolated tears of the triangular fibrocartilage: management by early arthroscopic repair. Repair of the triangular ligament in Colles' fracture. No effect in a prospective randomized study. Ulnar shortening combined with arthroscopic repairs in the delayed management of triangular fibrocartilage complex tears. Operative technique for inside-out repair of the triangular fibrocartilage complex.

My Wrist Before the Shortening
![]()
A bit more.....
I went into the doctors, I decided to try a more consrevative arthroscopic procedure. The last surgery I had on the arm cost me dearly, I am not one for going to the doc at all. I was awake the entire time, but I made sure as to have a sheet inbetween me and the "procedure". My arm was numbed, and then strapped to a board on my side. I was actually in a sitting position all the way, with my arm out and 90 degrees up. This was the weirdest sensation, something more like a torture chamber, but with a lot less pain, at least at the time.
Once I returned home, it started in, real pain. I didn't have too much really, yet it was very apparent that I had gone through with the first procedure. If this does not work, I'll have the decision to go on with the next challenge, what is called the "ulnar shortening procedure".
My
arm was then placed in a cast, giving some time to heal but all in all, it feels
better now than it has in well over 20 years. Even though I can't move my wrist
or elbow, I am now beginning to actually use my fingers, working out the muscles
that hopefully will become stronger and help my entire situation. I would much
rather have a few weeks in a cast, then to have my ulna shortened, a much more
serious procedure. Here is more on the complex itself, as well as additional
information on the Ulnar Shortening Procedure.
fibrocartilage complex abnormalities.
Hand-Clin. 1987 Feb. 3(1). P 31-40.
The distal radioulnar joint plays an intricate part in the function of the wrist and thus in the function of the entire upper extremity. The radius and hand move in relation to and function about the distal ulna. Significant loads are transmitted to the forearm unit through the distal ulna via the triangular fibrocartilage complex. The anatomic relationships between the distal radius and ulna and ulnar carpus are precise, and even minor modification in these relationships leads to significant load changes and resultant pain syndromes. Evaluation of a patient with ulnar wrist pain is, at best, difficult. Despite a careful and thorough history and physical examination and the use of sophisticated ancillary diagnostic studies, some patients with distal radioulnar joint and ulnar carpal complex problems remain diagnostic and therapeutic mysteries. These patients are best followed; exploratory surgery is rarely satisfying to either the patient or the surgeon. Armed with an understanding of the normal anatomy and biomechanics, the examination of such a patient and subsequent treatment should become a challenge that is rewarding for both patient and treating physician.
--------------------------------------------------------------------------------
Wafer distal ulna resection for triangular fibrocartilage tears and/or ulna impaction syndrome.
--------------------------------------------------------------------------------
Feldon P. Terrono AL. Belsky MR.
Journal of Hand Surgery - St Louis. [JC:ia9] 17(4):731-7, 1992 Jul.
Partial resection of the distal ulna (wafer resection) has been used to treat patients with symptomatic tears of the triangular fibrocartilage complex or mild ulna impaction syndrome. In this procedure, the distal 2 to 4 mm of the distal ulnar head is resected while preserving the ulnar styloid process and the ligaments attached to it. The triangular fibrocartilage is debrided, repaired, or partially excised as necessary. The procedure is contraindicated if there is more than 4 mm of positive ulnar variance. Thirteen wafer resections of the distal ulna were performed in 12 patients. All had good to excellent results after a minimum follow-up of 1 year. Wafer resection has specific advantages and avoids many of the potential complications of distal ulna recession and ulnar head resection for patients with the conditions described. The procedure is not indicated if instability or degenerative arthritis of the distal radioulnar joint is present or if there is carpal instability.
Technique: - longitudinal incision on the dorsal-ulnar side of the wrist; - the extensor retinaculum between the EDQ and ECU is incised; - the sheath of the ECU is left intact, eventhough this will make retraction of the tendon more difficult; - open the DRUJ capsule w/ a horseshoe shaped flap, leaving the radial side of the capsule intact; - the TFCC and ulnar styloid are identified; - the TFCC is protected, and a small osteotome is used to make a longitudinal cut 2-4 mm in depth along the radial side of the styloid process; - subsequently a thin oscillating saw is used to remove 2-4 mm from the head of the distal ulna; - the goal is to create 2 mm of negative ulnar variance; - ligametous repair and/or TFCC repair (or debridement) can be performed at this time; - capsular closure should include the peripheral edge of the TFCC, which allows the TFCC to be suspended w/ normal tension;
I wonder to myself, "is it really worth it ?". Actually I have had a somewhat easier time than I expected, what are friends for anyway ? Eating has been a challenge, every morning when I have to put on my shoes, I'm reminded of what is going on in my life. This is a very real thing, with very real consequences......I can only hope and pray it all works out for me. The biggest thing I've hated is all the sympathy and pity, man, I HATE that !
Well, this one is over.......I can now just reflect on the situations in which I faced along the way, this time. I will now endure many hours of rehab, making my arm back into the useful tool that it has always been. I will most likely have the ulnar shortening procedure later in the year. One thing I did learn from this is to keep the casted arm in the sling at least some! My shoulder really felt the brundt of the load, everything the wrist/elbow once did falls on the shoulder when it's in a cast like the one I had. Below is some additional info on the ulnar shortening teqniques, complete with some pictures.

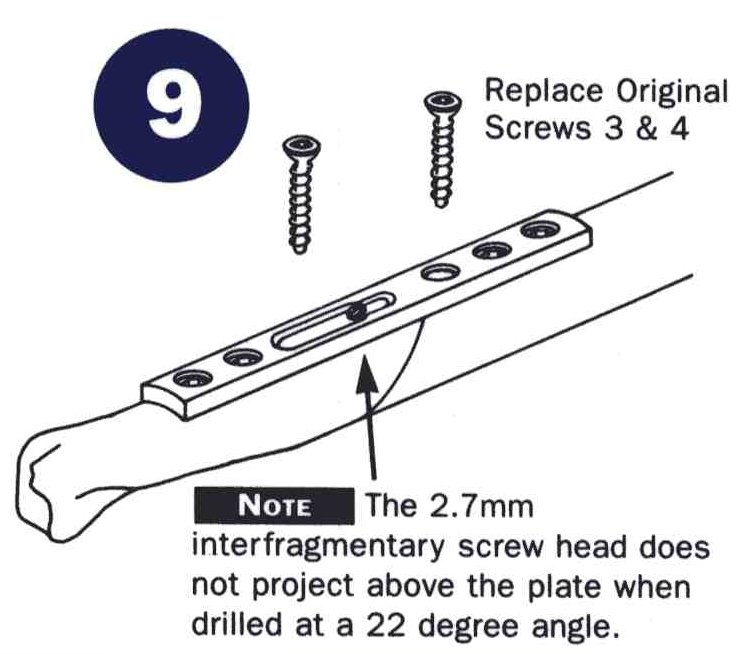
This is an extreme resection, a wafer procedure is much more conservative and a shortening procedure has the bone sliced and the center removed, pictures are below of this system.
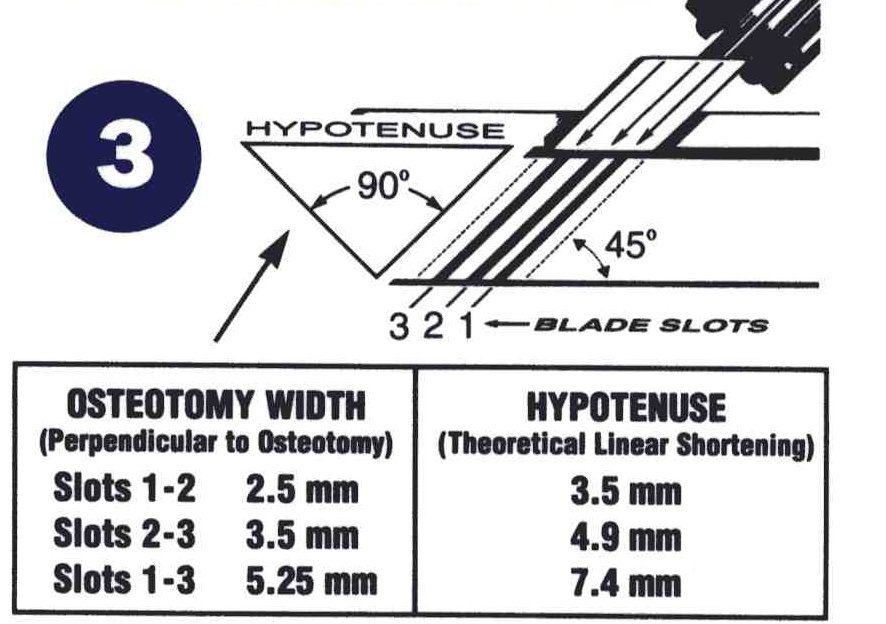
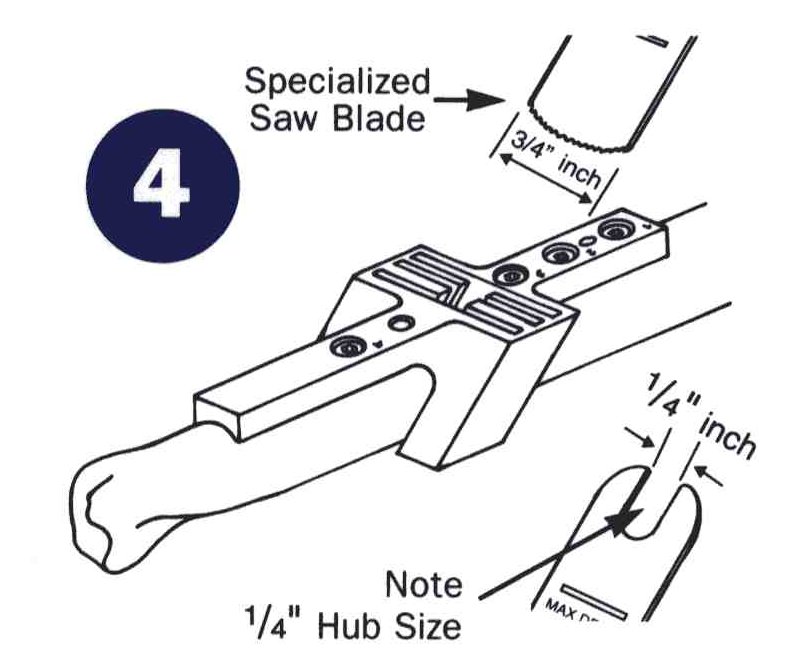
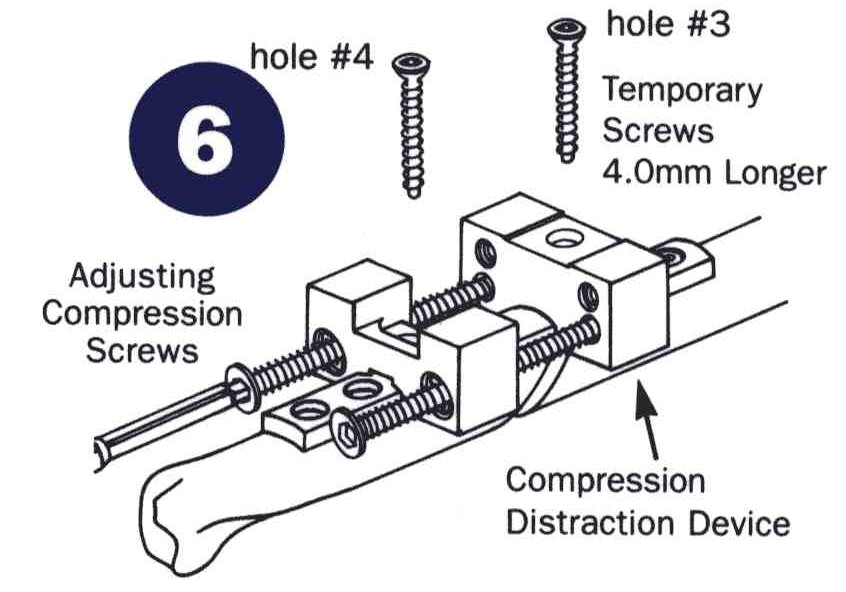
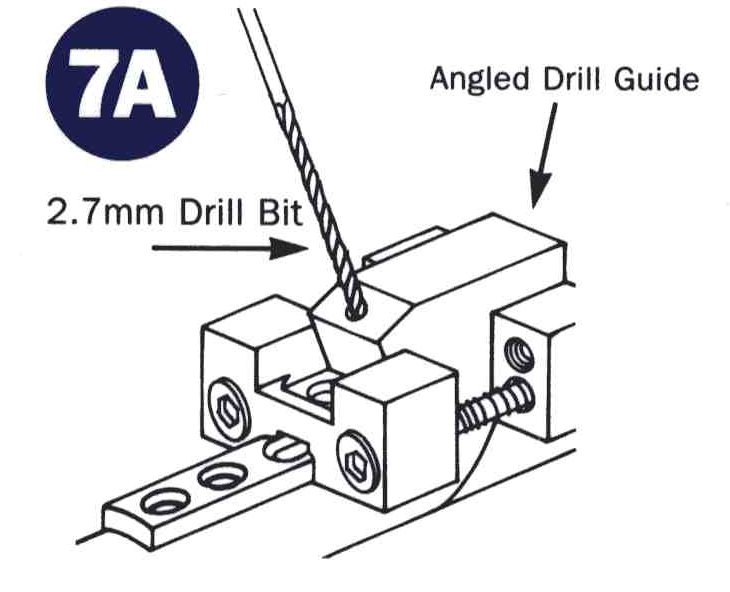
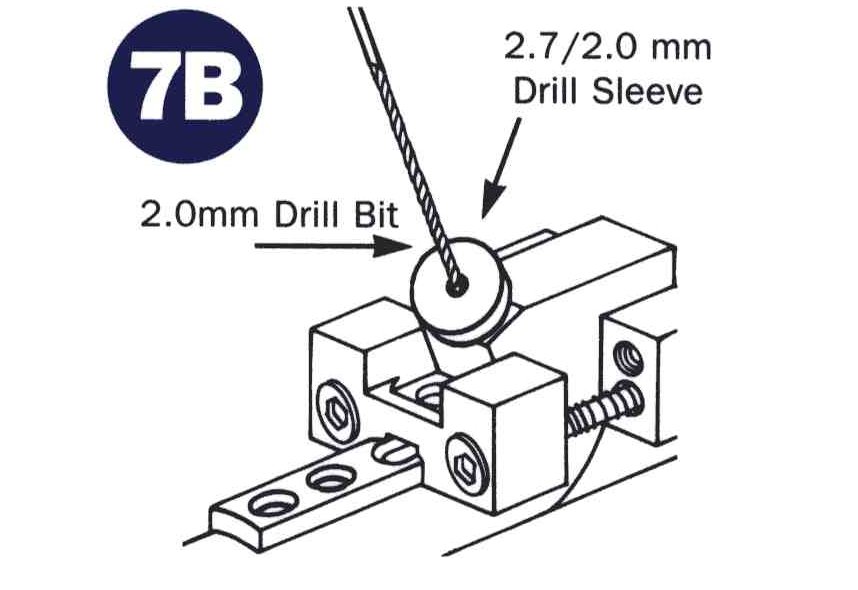
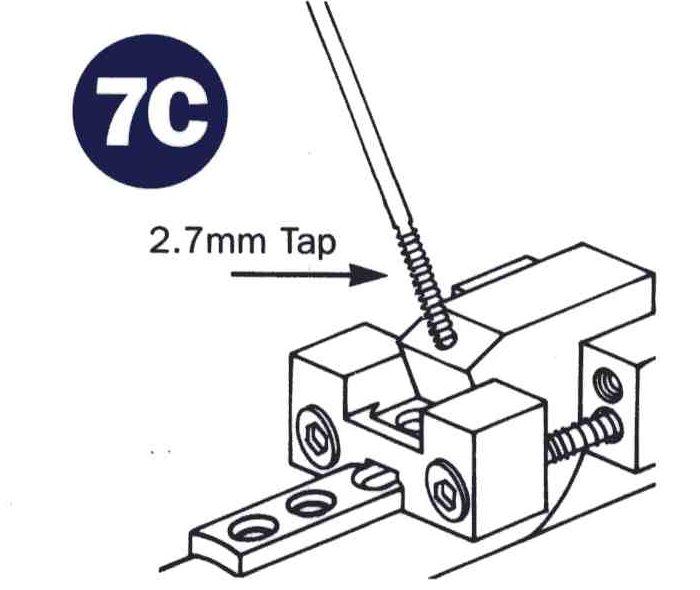
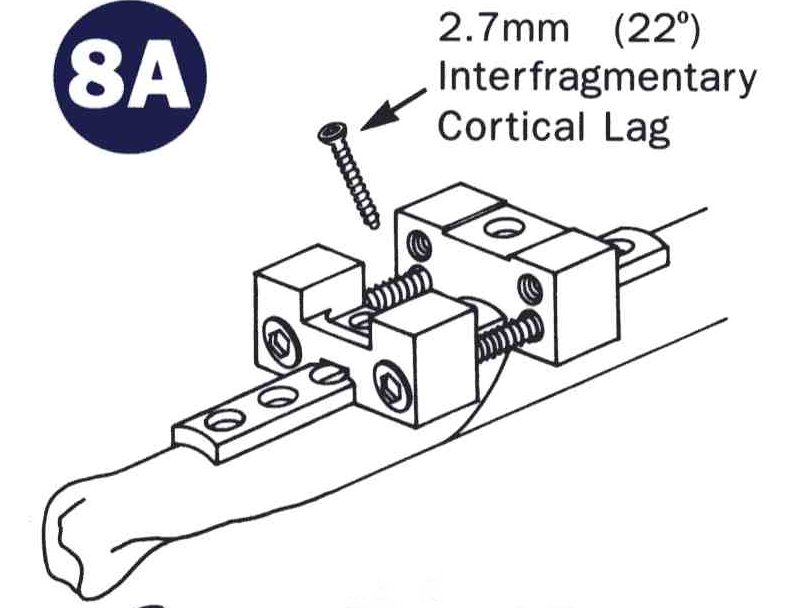
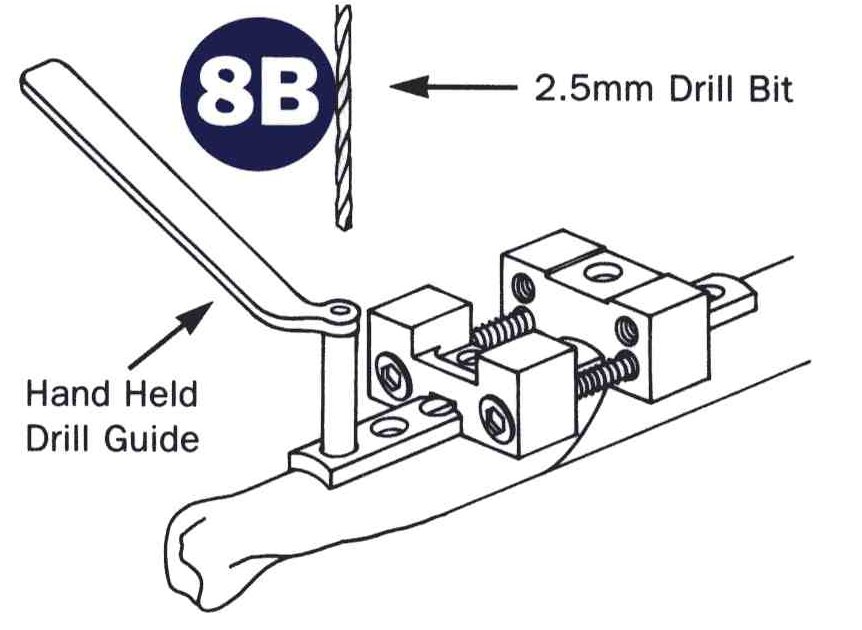
A few pics of the ulnar shortening tools required

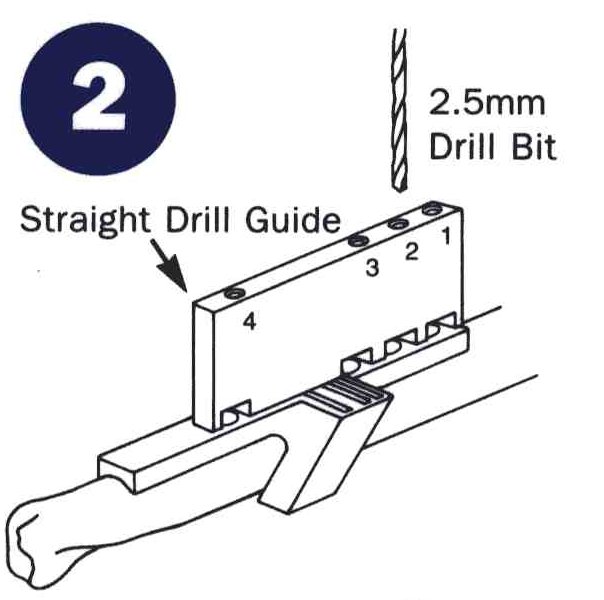

July 16th I underwent the ulnar shortening........
I knew it wouldn't be easy, I just didn't think it would be so hard. There was quite a bit of pain involved with the shortening,
somewhat more than I had expected. The procedure included the bone being cut through in two places with nearly an inch removed.
Immediately I did feel relief in the wrist area but now I was in a soft cast from my fingers to almost my armpit and the work was just
starting again. At first it was work just exercising my fingers, especially the pinky and ring fingers as they are directly effected
by the ulnar nerve. I also had some pain in my thumb which the doctor attributed to the years of bone grinding going on in my wrist.
After about a week resting in my easychair I was able to get back to work (at my desk job) and continue my rehab. I went to the doctor
to get the hard cast and he told me to expect about 10 weeks in the full cast with four more in a short version. At about two weeks I
began to not use the sling sp much and even to use my short arm to type a little. Ansering the phone at work took a toll as well and
my neck and shoulder started to feel the brunt of the load. Continuosly holding the phone on my good shoulder began to strain my neck
pretty good so I located and started using a headset which really helped a lot. After a few more weeks my short arm shoulder was
getting worse so it was back in the sling at work, the doctor told me to be very careful or the next surgery would be on the shoulder.
It was at eight weeks when I visited the doctor that they removed the full cast and I had more x-rays taken. Much to my surprise the
overwhelming cast was removed and with even more surprise no short cast at all! I was told to be careful and to start to work out
but not to overdo it. They should have mentioned that somewhat firmer as within a week I was back and in another cast...